Why write about prolapse management?
I was prompted to write this blog on best practice prolapse management for International Women’s Day because we had a patient report that both her GP and gynaecologist had made negative comments to her about the value of a pessary. This is disappointing in this day and age as a pessary is one of the many treatment options within the guidelines for prolapse management. Many women present to a physiotherapist with a special interest and training in pelvic health not wanting surgery and are excited to try a non-surgical option such as a pessary. Others are unsure and worry about what is involved and need time spent on comprehensive, thorough explanations.
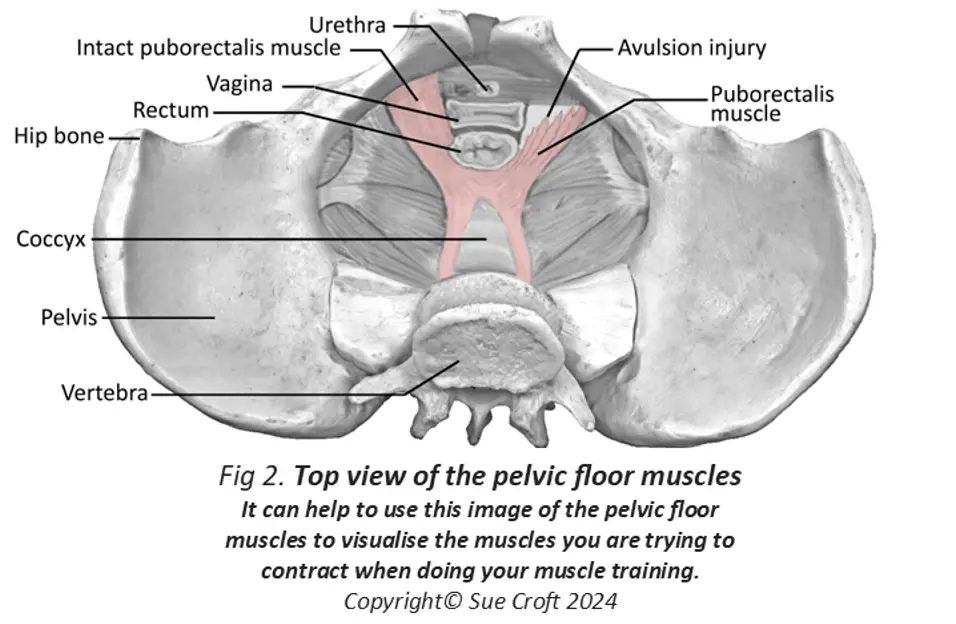
This patient’s treating physiotherapist assessed her thoroughly (tissue integrity, presence of pain, pelvic floor muscle strength, any sign of levator avulsion, degree of prolapse) and taught her:
- Pelvic floor muscle training and the importance of the knack
- Bladder and bowel education including position and dynamics of voiding and evacuation
- Discussed the potential value of a pessary fitting (for the immediate short term/or the medium term and/or the long term)
- Asked her to visit her GP to discuss having a speculum check to ensure it is safe to fit a pessary and to request a script for local oestrogen which is again on the treatment algorithm for prolapse treatment in a post-menopausal woman especially when having a pessary fitted.



There are many different varieties of pessaries
Sadly the patient received a very negative response from the GP about having a pessary fitted and the GP referred her to a gynaecologist who also was negative about the concept of a pessary and pushed for surgery. Her confidence waned about the pessary fitting and we will see what happens in the future.
Recommended Treatment for Prolapse
It is important that women know what the Australian Commission on Safety and Quality in Healthcare is promoting as the recommended treatment algorithm for pelvic organ prolapse (POP). Click on this link to read the full document.
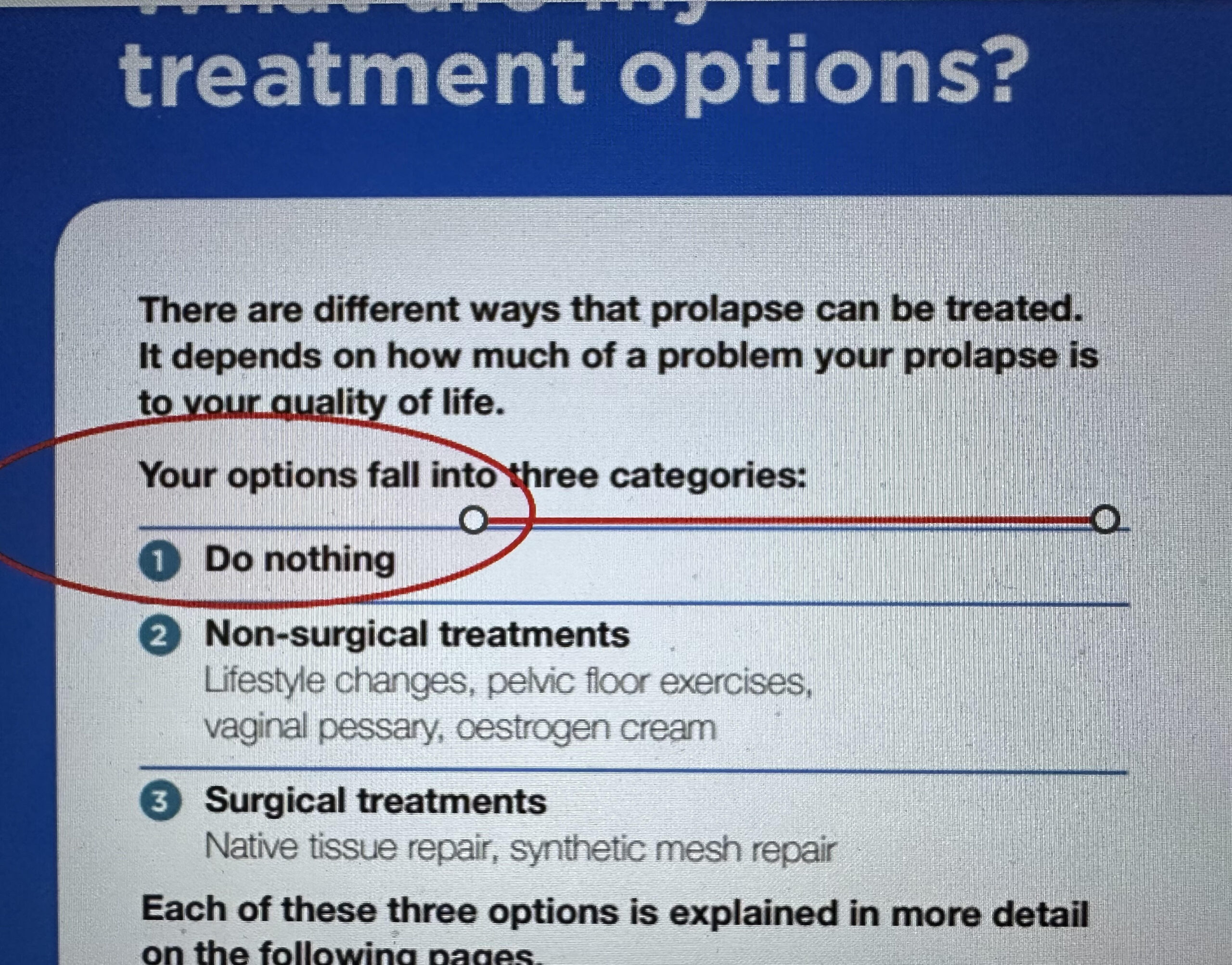
What this document succinctly says is:
Firstly:
- Do nothing (and I have written before that is silly when we know that symptoms can be significantly improved with conservative strategies that are offered by physiotherapists with a special interest and training in pelvic health)
- Non-surgical treatments (from a physiotherapist such as lifestyle changes, pelvic floor exercises, the knack and fitting a vaginal pessary which can also be fitted by a specialist such as a urogynaecologist or gynaecologist; and seeking a script for local oestrogen cream from a prescriber such as your GP)
- And finally should these strategies not manage the prolapse symptoms see a urogynaecologist or gynaecologist for surgical treatments (native tissue repair, synthetic mesh repair).
The physiotherapist’s treatment goals for this patient
The treatment plan devised by our physiotherapist was to fit the pessary to help with the bladder emptying (voiding dysfunction); to reveal any occult stress urinary incontinence (meaning leakage with cough or sneeze that is currently being hidden by the prolapse kinking the urethra); to relieve the uncomfortable bulge symptoms for the patient and to see if her low back pain would be helped by the pessary. Another value of pursuing a pessary in the short term, even if ultimately she will need surgery, is that if she reads the Australian Health Commission on Safety and Health Guidelines on prolapse management after she has surgery and the surgery has failed, she may wonder why a pessary wasn’t tried before surgery.
Why are Algorithms and Treatment Guidelines important for women?
Guidelines and algorithms are important for women to read and follow as it allows them to know what is evidence-based treatment for their particular condition.
There was a recent Four Corners programme which exposed the unfortunate treatment that many women have received for endometriosis at the hands of a Melbourne medical practitioner. He has allegedly operated over and over again on women with a diagnosis of endometriosis, but without evidence of endometrial tissue at histopathology. Worse still, the women were never told that there were no positive histopathology results or directed for other non-surgical treatment options for pelvic pain.
His treatment of one young woman was featured and the eight surgeries performed on her rendered her completely infertile at 25 years old. She had her uterus, and both ovaries removed with virtually no evidence of endometrial tissue at pathology. This not only has caused her to be infertile, it will have ramifications for the rest of her life due to losing her ovaries at such a young age.
It appears that important messaging was never offered or imparted to the women under his care – that evidence shows that the persistent pain suffered by women with a diagnosis of endometriosis is best treated in a multi-modal way involving not only a medical specialist (such as a specialised gynaecologist or a pain specialist) but also physiotherapists skilled in treating chronic pain, psychologists to manage stressors, dieticians for anti-inflammatory diet information to help the important gut microbiome and other health practitioners utilising other holistic strategies such as yoga, breath awareness and movement strategies.
Specialists well versed in this multi-modal approach of treating persistent pain have come out strongly since this Four Corners presentation encouraging women to understand the best treatment path they should be offered.
On International Women’s Day women need to be proactive around their health
Even a significant prolapse can be managed with a pessary
The point of this blog is to do some research before you embark on any health journey. Luckily we all have access to Google Scholar so we don’t have to just follow Instagram Influencers – we can read real articles on the topic and once you have done some reading then talk with your GP so you can confirm what you have read and challenge any negative bias that you may sense is happening.
Sometimes this is apparent around prescription of something as important to women as MHT (used to be known as HRT) or Menopause Hormone Therapy. This can be delivered to women as systemic treatments (patches, gels or oral tablets) or as local oestrogen (such as Vagifem or Ovestin cream). My whole generation missed out on the life-changing benefits of systemic hormones (dementia prevention, maintenance of bone density and heart benefits) due to poor research around these medications and increased risk of breast cancer for which the narrative has been difficult to change for many years. Finally after many decades, the Black Box warning for hormone treatments has been removed.
It doesn’t help that there is so much health misinformation around (and unfortunately some is coming from highly positioned politicians in other countries). It can all be very confusing and misleading.
Medical Misogyny in Health Care
Women’s Health has suffered from poor research for many years because for much of the basic science research, male rats have been used rather than female rats which has led to many issues, including adverse drug reactions in women. Historically medical studies have excluded female participants and collected research data from males and generalized it to females. The gender gap in medical research, alongside overarching misogyny, results in real-life disadvantages for female patients (for example in cardiovascular research and the different presentations women have with heart attacks). (1) Here is an interesting article on Sex Inequalities in Medical Research
Conclusion
I find that on this 2026 International Women’s Day (IWD) I have feelings of can I be bothered anymore celebrating this day? Every day I wake up and hear terrible statistics about violence against women around the world and particularly in Australia; I read about horrific case studies in USA with the anti-abortion laws that literally lead to women dying; and I know there are many countries that have restrictive, patriarchal laws that limit agency, education, and reproductive rights of women and girls.
After years of promoting IWD, I have decided to think local and state the case for something I can do something about. I am dedicating this year to promoting the value of pessaries for vaginal prolapse to encourage women to lift weights, run and exercise with gay abandon because they have had a successful pessary fitting. I encourage my pelvic health colleagues to continue to do this. Fitting a pessary is time consuming, it is frustrating at times when you hit hurdles such as someone who has significant pelvic floor muscle trauma and 8 pessaries haven’t worked – try a 9th – it may be the one that gives your patient ten more years before she needs surgery. We all have to continue to educate the community and our medical colleagues that having a go at fitting a pessary is very worthwhile.
It truly has been and is the most fabulous life-changing thing I have learnt in my long career.
References:
(1) Merone L, Tsey K, Russell D, Nagle C. Sex Inequalities in Medical Research: A Systematic Scoping Review of the Literature. Womens Health Rep (New Rochelle). 2022 Jan 31;3(1):49-59. doi: 10.1089/whr.2021.0083. Erratum in: Womens Health Rep (New Rochelle). 2022 Mar 16;3(1):344. doi: 10.1089/whr.2021.0083.correx. PMID: 35136877; PMCID: PMC8812498.
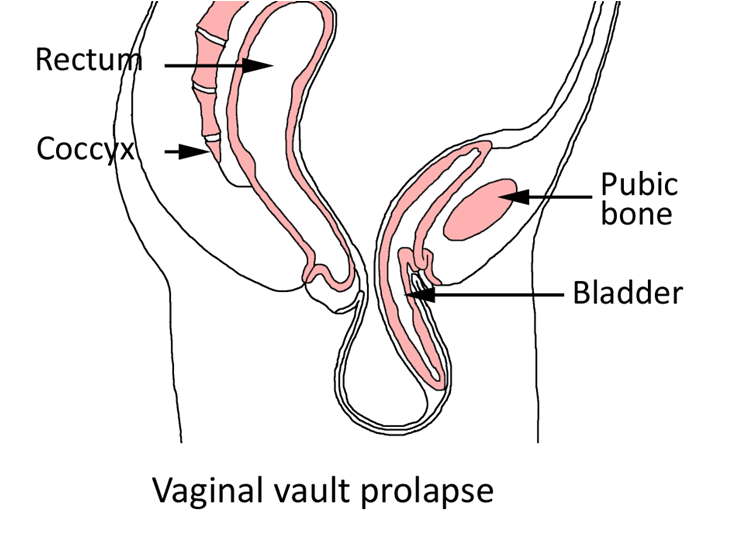
Images taken from my books Pelvic Floor Essentials Edition4 and Pelvic Floor Recovery: Physiotherapy for Gynaecological and Colorectal Repair Surgery Edition5
Excellent information. Thank you, Sue. I have the pentagram-shaped pessary fitted by a member of your practise and also a replacement a year later. I go to another pelvic floor physio now as she is a bit closer to Beaudesert. I am hoping she can access a new pessary of the same kind for me when I see her in a few weeks.
Thanks, Margaret.
Thanks Margaret for leaving a comment. And yes distance is sometimes a problem. Good luck
Sue
Fabulous blog, Sue Croft. I completely agree about pessary use, please continue to champion pessary use!
Whenever a woman is diagnosed with prolapse, my advice is simple: consider using a pessary while you consider your options. It can help you manage symptoms while you decide what to do next — whether that’s choosing a pelvic exercise device, lifestyle changes, waiting for a physio appointment, or even preparing for surgery, or all of the above. Manage the prolapse you have.
I’m not a medic, but after more than 30 years of speaking with women about pelvic health, I’ve seen how valuable this conservative treatment can be. Pessary use is often underestimated, yet it can make a real difference.
Let’s make sure women know they have options — and the time to choose what’s right for them – IWD and every day in between. Thank you Sue Croft. x
Hi Stephanie
Great to read your comment. That is it in a nutshell! Giving a pessary a go (as well of course as the usual advice and exercises that physios give) means you have tried everything and surgery is the next step. But if a women isn’t given a clear explanation about the value or purpose of a pessary, or is rushed with just one option tried and it falls out, then they can easily get a poor opinion of a pessary – which is sad.
I hope you are well and thank you for taking the time to post a comment. Sue x
This is such a thoughtful and educational post Sue!!! As a pelvic health physiotherapist in Canada who fits pessaries I echo your concerns. I have so many patients that tell me they ‘get their lives back’ once they have a pessary that works for them….and yet I have some patients whose primary care physician advises them against it!!! I have had patients in their 70s who have been told they are too old for a pessary and others in their 40s who have been told they are too young!!!!! Now I am doing training for primary care physicians all about pessaries so that I can say I am trying to change the messages and the knowledge!!
Thanks Kristen. Lovely to hear from you. Yay to Canadian Pelvic Health physical therapists helping their clients also and spreading the global message.