
That is a literal photo of a full rubbish bin of years of ‘post it’ notes and articles I had sitting waiting for me to read.
I have spent today cleaning up all the post-it notes filled with new things someone had told me, nice little quotes and other titbits that I have as a pile on my desk at home (which was quite mountainous) and numerous scholarly research articles printed out that I had saved to read on a rainy day. Today was that day and I have a tremendous sense of satisfaction that I have actually gone through the pile, filled the bin and found some very interesting reminders and written them in one book to look at another day…….
In my pile of recent pelvic health articles were some fabulous ones that had great new research immediately able to be implemented in clinic (e.g. exercise guidelines in pregnancy), but I also came across a printout of one that was published in the Canadian Physiotherapy Newsletter last year of an interview that Katie Kelly did with me about my career.
I have decided I would post it in my blog for interest (and as a self-indulgent memory for me).

Katie Kelly PT (Canada)
The questions were posed by Katie Kelly PT (Canada) who is the Editor of the Newsletter. I thank Katie again for the interview.
Question 1: Why are you considered a guru in the field of pelvic floor physio, and in particular how have you developed your expertise on guiding patients through the post-operative period of pelvic surgeries?
To be honest, I do dislike the word ‘guru’. I would never use that word to describe myself, but would prefer that I am described as passionate, engaged and responsive to changes in the area of pelvic health over my career. Graduating in 1977, I have been a practising physiotherapist for 49 years continuously and 38 of those have been in women’s and pelvic health – so I have been doing this for a long time.
Across those many years I have seen lots of presentations of different conditions with patients and what I’ve learnt is most importantly listen to the patient, believe what they’re saying to you and be curious about what could be happening if it doesn’t fall into certain parameters of what you have learned in your courses.
I do love reading anything about pelvic health, so I read lots of journal articles and books. Over the years, I’ve also attended many national and international conferences, and I think that’s important for new pelvic health physiotherapists to understand about the value of engaging and networking with your peers from around the world.



ICS Florence 2016 with Helen and Jenny and Michelle Lyons and IUGA The Hague 2023 with Alex



IUGA The Hague 2023 with Dr Peta Higgs Urogynaecologist & Annie, Claire, Fiona-wonderful Aussie Pelvic Health Physios and Professor Suzanne Hagen (Glasgow) at CFA 2024, Brisbane.
I’ve been lucky enough to develop very good relationships with urogynaecologists and obstetricians and gynaecologists, who have gone on to become good friends. I have two of the best urogynaecologists in the world on speed dial, so I can always ask their opinion or a question if I have one.


Professor Judith Goh and Professor Hannah Krause at the O&G World Congress 2016 (Brisbane) and at the Hamlin Fistula Hospital in Ethiopia
My interest in the post-operative advice and guidance that a physiotherapist can give a patient has developed due to their incredible support of me over the years. They are very pro-physiotherapy and try actively to not operate until it’s absolutely necessary. This has given me the confidence to say that physiotherapy is very important in the pre-and post-op treatment of pelvic health patients to enhance the surgical outcome for that patient.
I also got tired of writing out the same instructions over and over for my pre/post op patients, hence the idea for the book emerged. A life experience of my own in 2011 (a discussion that an abnormal ultrasound could be uterine cancer) gave me the jolt to start writing then and there, that weekend! Fortunately, it was not the worst-case result – all was good, but the book was started and finished 8 weeks later and now in 2025, Pelvic Floor Recovery: Physiotherapy for Gynaecological and Colorectal Repair Surgery is up to Edition 5.
Relationship building with all health professionals is the best advice I can give any young physiotherapists starting out. Being mentored by experienced physios is also very useful.
(Author note: You can find Sue’s above-mentioned book Pelvic Floor Recovery Bookshop | Pelvic Floor Recovery, here.)
Question 2. Which of your many publications, handouts, podcasts, research, or webpages would you recommend that pelvic floor physiotherapists check out?
I love my pelvic health blog, which I have relocated over to the book website www.pelvicfloorrecovery.com when I sold my practice in March 2024. Years ago, I discovered how wonderful it is to send evidence-based information around the world via the internet and help many women (and men and children) with their various issues, as well as one patient at a time in the rooms.

I have published over 480 blogs now and have never lost the passion for writing them. Everything I write is written in a conversational way so that it is easy to understand for the reader and health professionals alike. My other book is Pelvic Floor Essentials Edition 4 which is the book I would recommend to adolescent girls and women who haven’t had children, and for pregnant and post-natal
women particularly those in their recovery phase, right up to the post-menopausal woman.
Once women are around 60, I often encourage them to purchase Pelvic Floor Recovery: Physiotherapy for Gynaecological and Colorectal Repair Surgery Ed 5,
the surgical book, but just skip reading the surgical chapters. It is the most up-to-date book (2024) with comprehensive bladder, bowel, prolapse and pain information without the ante/post-natal information which isn’t necessary for the over 60 cohort anymore.
We are blessed these days with a plethora of wonderful opportunities to learn and engage with experienced pelvic health physiotherapists via the various Facebook groups, podcasts and even Instagram social media. I have done quite a few podcasts with Michelle Lyons, Lori Forner and Fiona Rogers has a fabulous podcast on pelvic health products.



Dr Lori Forner teaching us all her pelvic ultrasound wisdom (pictured with Dani one of our lovely physios at Active Women’s Physiotherapy, Highgate Hill) and Tamara Woods Physio & her Pelvic Health Community.
I know these clever women well, and respect them so much, and we always have a ball when we chat. I did particularly enjoy talking to Lori, Jo Murdoch and Tamara Woods about burnout in pelvic health physiotherapy and the many different ways pelvic health physiotherapists can source their learning to upskill into pelvic health.
Question 3: With your experience in this field, what is something that you might do in a patient assessment, that may not be standard practice for new pelvic floor physiotherapists?
I did Carolyn Vandyken’s course on the Biopsychosocial Management of Pelvic Pain in 2020 and having done four of Lorimer Moseley and Dave Butler’s Explain Pain courses over 12 years – all of Carolyn’s work using screening questionnaires tied in nicely with my love of their pain neuroscience education.
I love diving deeper into what is going on for the patient in their home, work, and leisure life. We know that anxiety levels over the past 5 years have escalated enormously, and this has a profound effect on any pelvic health issue, regardless of whether it is pain or urinary leakage or prolapse that is bothering the patient. Once identified, the patient can then see that if they are not using strategies to better manage any stress and anxiety, their pain or urinary or faecal incontinence may not improve to an optimal level.
I also want to stress how important it is for the new physiotherapist to avoid using excessively technical terms and scary language when explaining their assessment and diagnosis to the patient. Always keep the patient calm while explaining your strategies to them, rather than trying to look overly clever.
Question 4. Can you offer one or two treatment techniques, tips or exercises, that you find invaluable for the post-operative pelvic floor population? Why are these so helpful to your patients?
My biggest piece of advice is for all physiotherapists to strongly advocate for their patients regarding the advantages of pre- and post-op physiotherapy. As our readers are aware, the evidence in the literature, such as RCT’s conducted by Nyhus (2020, 2021), Duarte (2020) and Jelovsek (2020) into pre-, peri- (from prior to and after surgery), and longer-term physiotherapy as a treatment intervention for gynaecological surgical repair, is somewhat disappointing. Reason being, they fail to
show a significant difference in outcomes of surgery with physiotherapy treatment. These results diminish the importance of an individualised approach to treating patients and do not necessarily acknowledge the psychosocial dimension of a pelvic health physiotherapist’s consultation.
In clinic, these patients are often anxious and unsure about surgery, and increasingly, pelvic health physiotherapists are adopting a biopsychosocial approach with their management pre-operatively. This helps with calming and reassuring patients that they have fully explored the conservative strategies, and surgery is the logical next step.
Women may also carry psychological trauma from their early formative years and any vaginal birth injuries that happened years before, therefore it is important to approach any education, examination, and treatment of the woman in a trauma-informed way.



Pelvic Floor Recovery: Physiotherapy for Gynaecological and Colorectal Repair Surgery Ed 5 provides a framework for patients especially when they cannot access a pelvic health physio where they live
A pre-and post-op treatment programme with a physiotherapist provides a framework for the patient, with the physiotherapist playing a valuable role as a support person on this journey. Holistically supporting a woman following surgery in returning to exercise in a ‘pelvic floor friendly way’ is as equally important as achieving a good anatomical result.
Over the past decade, as awareness of pelvic health conditions has grown, some women have become fearful that exercise will worsen their pelvic organ prolapse (POP) and stress urinary incontinence (SUI). This is partly due to advice that has blanket recommendations from health professionals and social media alike, rather than providing an ‘individualised medicine approach’ to exercise prescription for each individual woman.
If women restrict or stop exercising due to pelvic floor dysfunction, significant ramifications for their general health such as bone density depletion, poorer cardiovascular status, sarcopenia, mental health dysfunction and overall wellness may occur. If a woman is afraid to exercise following her POP repair surgery, her general health and wellbeing will suffer. Reassuring the patient that return to exercise can be modified in a safe way will help make them feel supported in their quest to return to exercise, work, and sexual intimacy.
Question 5: Aside from your own resources, are there any other websites, books, podcasts, etc, that you would recommend to your patients, or other physiotherapists that could help support patient recovery?
I have always been a member of the Continence Foundation of Australia which is now renamed as Continence Health Australia (CHA), the International Urogynaecological Association (IUGA), and the International Continence Society (ICS). Together with our own national physiotherapy association, the Australian Physiotherapy Association (APA) and the special interest groups relevant to my area of work, it all adds up from a cost point of view.
However, belonging to the peak organisations around pelvic health issues means you are reading all the relevant research that keeps our profession up-to-date and abreast of change. As a member of ICS, you can purchase the 7th ICI, which is the seminal document with respect to all pelvic health information and travelling to countries in Europe for an international conference is a nice bonus.
We are lucky in Australia to have Taryn Hallum present our education via the Women’s Health Training Associates. Her deep dive into research keeps us all up to date and improves our critical thinking skills which is so important for our area.
The UK Clinical Guideline: Best Practice in the Use of Vaginal Pessaries is important for anyone working in pessaries to adhere to. Here is the link.
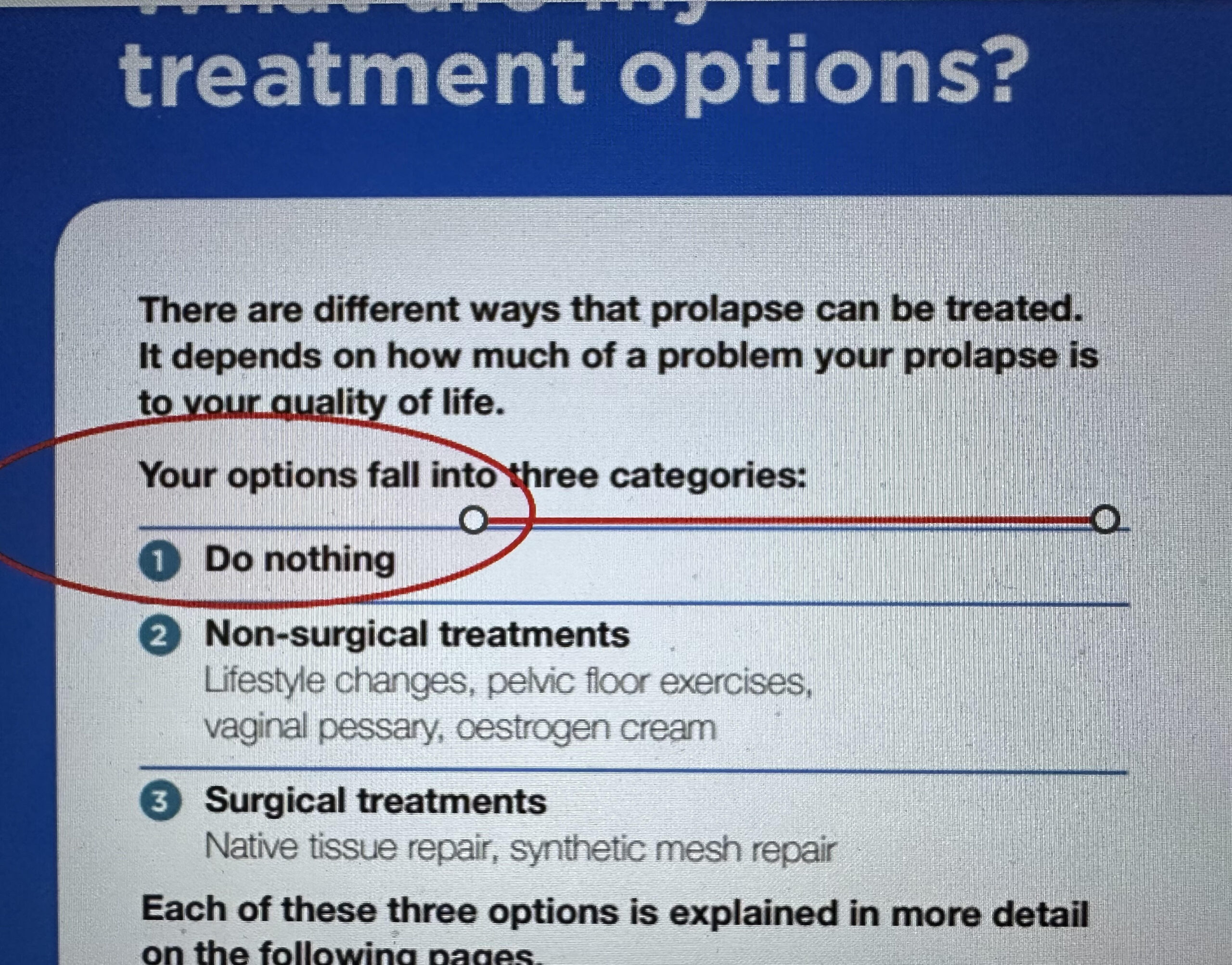
I would also recommend the documents on SUI, POP, Transvaginal Mesh and 3rd and 4th Degree Perineal Tears Clinical Care Standard we have in Australia from the Australian Commission on Quality and Safety in Health Care. Click on the links below.
Urinary Incontinence
Sue Croft OAM, PT (B Physiotherapy University of Queensland, 1977)
Contact Information: sue@pelvicfloorrecovery.com
X (Twitter): scroftpf
Instagram: pelvicfloorrecoverybooks (and scroftpf)
Facebook: Pelvic Floor Recovery Books and scroftpf
TikTok: @scroftpf
Bio: Sue Croft is a physiotherapist in private practice in Brisbane, Australia with a special interest in Pelvic Health Physiotherapy. Sue has worked in Women’s, Men’s and Children’s pelvic health since 1988. Sue has written three books on pelvic health and is a passionate blogger on pelvic floor dysfunction. She actively encourages women to seek help from a pelvic floor physiotherapist for any issues and promotes education for the bladder, bowel, and pelvic floor through social media. Sue was awarded the Order of Australia Medal in 2023 for her services to community health as a physiotherapy.